


To evaluate the pH value of children's antibacterial soaps and syndets used in children's baths and verify whether there is information regarding pH on the product label.
MethodsQuantitative, cross-sectional, analytical observational study that included ninety soap samples, both in bar and liquid presentations, as follows: 67 children's soap (group 1), 17 antibacterial soaps (group 2), and 6 syndets (group 3). Each sample had its pH measured after 1% dilution. In addition to descriptive statistics, the Pearson–Yates chi-squared test and Student's t-tests were applied, considering the minimal significance level of 5%. The Wilcoxon–Mann–Whitney test, Fisher's exact test, and the Kruskal–Wallis test were used for inferential statistics.
ResultsThe pH levels varied considerably between liquid and bar presentations, with lower levels (4.4–7.9) found for the liquids (p<0.05). Syndets showed pH levels close to the ideal (slightly acid) and the antibacterial soaps showed the highest pH levels (up to 11.34) (p<0.05). Only two of the soaps included in the study had information about their pH levels on the product packaging.
ConclusionsKnowledge of the pH of children's soap by doctors and users is important, considering the great pH variability found in this study. Moreover, liquid soaps, and especially syndets, are the most recommended for the sensitive skin of neonates and infants, in order to guarantee skin barrier efficacy.
Avaliar o pH dos sabonetes infantis, antibacterianos e sindets habitualmente utilizados em crianças; bem como verificar se há no rótulo desses produtos informação sobre seu pH.
MétodosEstudo observacional, analítico, transversal e quantitativo, que incluiu 90 sabonetes nas apresentações em barra e líquida, sendo 67 infantis (grupo 1), 17 antibacterianos (grupo 2) e 6 sindets (grupo 3). Procedeu-se a mensuração do pH das amostras após diluição a 1%. Além da estatística descritiva, foram usados os testes de Qui quadrado Persons/Yates e teste T de Student,com nível de significância mínimo de 5%. Para a estatística inferencial, foram usados os testes de Wilcoxon–Mann–Whitney, exato de Fisher e Kruskal–Wallis.
ResultadosO pH variou consideravelmente entre as formas líquida e em barra, com pHs menores (de 4,4 a 7,9) nos líquidos (p<0,05). Os sindets mostraram pHs próximos ao ideal (levemente ácidos) e os antibacterianos apresentaram os maiores pHs (até 11,34) (p<0,05). Apenas dois dos sabonetes analisados apresentavam no rótulo a indicação do pH.
ConclusõesA observação do pH dos sabonetes infantis pelos médicos e usuários é importante, haja vista a grande variabilidade de valores de pH encontrados. Além disso, os sabonetes líquidos, e especialmente os sindets, são os mais recomendados para uso em recém-nascidos e lactentes com pele sensível, de forma a garantir a eficácia da barreira cutânea.
The skin of newborns (NBs) has indispensable functions for their development: it acts as a protective barrier,1 helps thermoregulation, exchanges gases, maintains hydration, and contributes to innate immunity.2 Additionally, its mildly acidic pH provides additional protection against pathogens.1 The disruption of this natural barrier allows opportunistic microorganisms to affect infants with bloodstream dissemination, especially in premature infants due to immunological system immaturity.3 Studies indicate that the infant's skin continues to develop for up to 12 months after birth4,5 and that it differs from the adult skin in several aspects, such as composition, structure, function, and its susceptibility to infections.4,6,7
The potential of hydrogen (pH) of the slightly acid skin is an important factor in the protection against microorganisms – it is essential for the epidermal barrier maturation and repair processes.8 In adults and adolescents, skin pH is <5 (pH<5). In the thinner skin, especially in preterm infants, the pH tends toward neutral, resulting in significant loss of defense against microbial proliferation, as well as higher transepidermal water loss.9 At birth, a full-term NB's skin has a pH ranging from 6.3 to 7.5.10,11 Within the first 2 weeks of life, the pH drops to approximately 5.11 Between the second and fourth weeks of life, the pH becomes gradually acid, ranging from 4.2 to 5.9, depending on the area of the body, with higher values found in the axillary, genital, and interdigital areas.12
Bath time is a moment of relaxation and mother–child interaction, in addition to being indispensable for the maintenance of skin hygiene and health.13 The bath keeps the skin free of irritants (saliva, nasal secretions, urine, feces, and fecal enzymes), dust, and microorganisms.1 According to the World Health Organization (WHO), it is recommended that the NB be given the first bath 6h after birth.9 It has been suggested that a bath given with only water is the least harmful method of cleaning the NB, which has been adopted in the national postnatal care protocols in many countries, including the United Kingdom.9 However, the buffering capacity of water has been questioned, as it can increase skin pH from 5.5 to 7.5. Moreover, the use of water alone was identified as an ineffective cleaning agent, as it does not remove oily substances such as feces and sebum.14,15 American guidelines recommend the use of lukewarm drinking water, with the option of associating a mild cleaning product with a physiologically adequate pH (5.5–7.0).14
It is believed that the repeated use of cleaning agents can alter the skin surface pH in the long term.12 Traditional soaps have an alkaline pH, which can destroy the skin lipid layer9 and elevate skin pH above 8.0, leading to skin dryness and irritation.12,14,16–19 A pH of 7.5 is capable of increasing skin protease activity and inhibiting lipid lamellae synthesis, leading to a breakdown of the skin barrier.14
The “syndets”, a term derived from “synthetic detergent”, are formulated from synthetic surfactants that have good detergent effect, with neutral or slightly acid pH, and cause less irritation.9 Studies show that taking a bath using this type of soap is comparable or even superior to a bath with water only.20
A good cleaning product for NBs must have a pH close to 5.5 and some buffer capacity to maintain the pH close to that level.14 The cosmetic industries offer a great variety of such products and classify them as “mild”. However, there is no international criterion to establish the mildness of cleaning agents, and often, various products advertised as adequate for sensitive skins exhibit significant irritative effects.21
Thus, the aim of this study was to evaluate the pH of children's soaps, antibacterial soaps, and syndets commonly used to bathe children and infants, in order to verify whether they are slightly acidic and, therefore, consistent with the maintenance of the water–lipid mantle and barrier function and, secondly, to determine whether the labels of these products have information about their pH.
MethodsThis was an observational, analytical, cross-sectional, quantitative study. Products from all brands (liquid or bar) of children's soap were obtained, antibacterial and syndets found at points of purchase (supermarkets, drugstores, and cosmetic stores) located within 7km of Hospital de Clínicas, located in downtown Curitiba, state of Parana, Brazil. These samples were paid for using the researchers’ own funds, in order to avoid any conflicts of interest. Ninety types of soaps were analyzed (62 bars and 28 liquid soaps), divided into three categories, including 67 children's soaps, 17 antibacterial soaps, and six syndets. These groups were further divided into five categories according to pH ranges: pH<5; between 5 and 5.9; between 6 and 6.9; between 7 and 7.9; and ≥8.
The pH of all the soap samples was measured using a pHmeter® (Hanna Instruments, model H19321, TX, USA) at a dilution of 1% in distilled water (pH 9.1). A comparison between 1% and 10% dilutions was performed and it was verified that pH values remained the same. Thus, due to the fact that smaller volumes are easier to use, the 1% dilution was chosen.
Data were stored in a Microsoft Excel® spreadsheet and evaluated using R® software, version 3.0.2 (Microsoft®, Washington, USA). Summary measures used in descriptive statistics were mean, standard deviation, median, minimum and maximum values, and frequencies, depending on the type of the studied variable. The Pearson–Yates chi-squared test and Student's t-test were applied, considering the significance level of 5%. The tests used for inferential statistics (data comparison) were the Wilcoxon–Mann–Whitney test, Fisher's exact test, and the Kruskal–Wallis test.
This study did not require the approval by the ethics committee, as it did not involve human subjects, but only the biochemical analysis of soaps; opinion No. 064.2012.
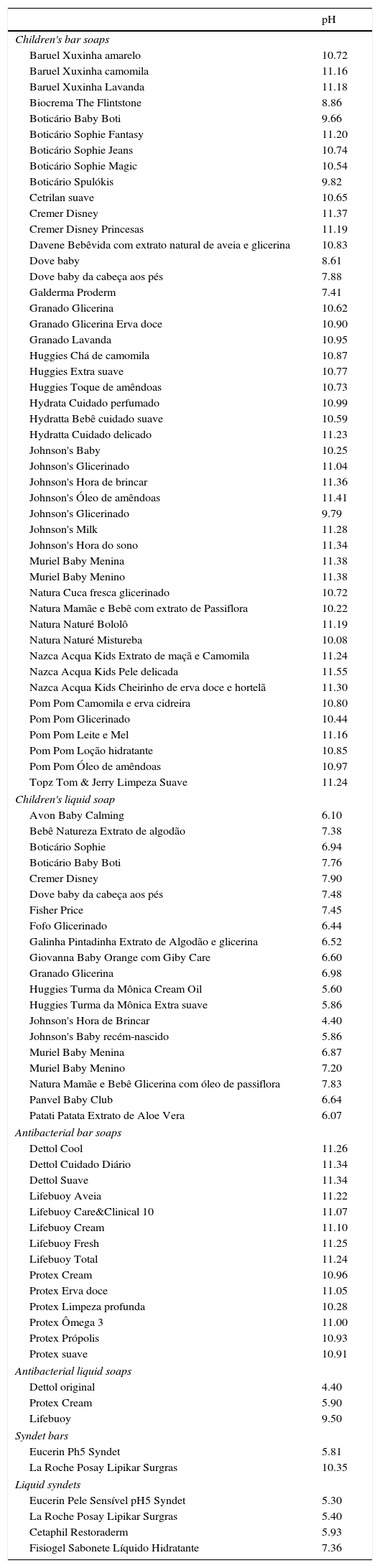
ResultsThe pH of the soaps ranged from 4.4 to 11.5, with a median of 10.7. Two (2.2%) had pH<5, 8 (8.8%) soaps had pH between 5 and 5.9, 9 (10%) had pH between 6 and 6.9, 10 (11.1%) had pH between 7 and 7.9, and 61 (67.7%) had pH>8.
In the group of children's soaps, 47 were bars and 20 were liquid soaps (Table 1). Only one of bar soaps had pH<8 (2.2%). Among the liquid soaps, 1 (5%) had pH<5.0; 3 (15%) had pH from 5.0 to 5.9; 9 (45%) had pH from 6.0 to 6.9; and 7 had (35%) pH from 7.0 to 7.9.
Soaps according to their group, presentation, and potential of hydrogen (pH).
| pH | |
|---|---|
| Children's bar soaps | |
| Baruel Xuxinha amarelo | 10.72 |
| Baruel Xuxinha camomila | 11.16 |
| Baruel Xuxinha Lavanda | 11.18 |
| Biocrema The Flintstone | 8.86 |
| Boticário Baby Boti | 9.66 |
| Boticário Sophie Fantasy | 11.20 |
| Boticário Sophie Jeans | 10.74 |
| Boticário Sophie Magic | 10.54 |
| Boticário Spulókis | 9.82 |
| Cetrilan suave | 10.65 |
| Cremer Disney | 11.37 |
| Cremer Disney Princesas | 11.19 |
| Davene Bebêvida com extrato natural de aveia e glicerina | 10.83 |
| Dove baby | 8.61 |
| Dove baby da cabeça aos pés | 7.88 |
| Galderma Proderm | 7.41 |
| Granado Glicerina | 10.62 |
| Granado Glicerina Erva doce | 10.90 |
| Granado Lavanda | 10.95 |
| Huggies Chá de camomila | 10.87 |
| Huggies Extra suave | 10.77 |
| Huggies Toque de amêndoas | 10.73 |
| Hydrata Cuidado perfumado | 10.99 |
| Hydratta Bebê cuidado suave | 10.59 |
| Hydratta Cuidado delicado | 11.23 |
| Johnson's Baby | 10.25 |
| Johnson's Glicerinado | 11.04 |
| Johnson's Hora de brincar | 11.36 |
| Johnson's Óleo de amêndoas | 11.41 |
| Johnson's Glicerinado | 9.79 |
| Johnson's Milk | 11.28 |
| Johnson's Hora do sono | 11.34 |
| Muriel Baby Menina | 11.38 |
| Muriel Baby Menino | 11.38 |
| Natura Cuca fresca glicerinado | 10.72 |
| Natura Mamãe e Bebê com extrato de Passiflora | 10.22 |
| Natura Naturé Bololô | 11.19 |
| Natura Naturé Mistureba | 10.08 |
| Nazca Acqua Kids Extrato de maçã e Camomila | 11.24 |
| Nazca Acqua Kids Pele delicada | 11.55 |
| Nazca Acqua Kids Cheirinho de erva doce e hortelã | 11.30 |
| Pom Pom Camomila e erva cidreira | 10.80 |
| Pom Pom Glicerinado | 10.44 |
| Pom Pom Leite e Mel | 11.16 |
| Pom Pom Loção hidratante | 10.85 |
| Pom Pom Óleo de amêndoas | 10.97 |
| Topz Tom & Jerry Limpeza Suave | 11.24 |
| Children's liquid soap | |
| Avon Baby Calming | 6.10 |
| Bebê Natureza Extrato de algodão | 7.38 |
| Boticário Sophie | 6.94 |
| Boticário Baby Boti | 7.76 |
| Cremer Disney | 7.90 |
| Dove baby da cabeça aos pés | 7.48 |
| Fisher Price | 7.45 |
| Fofo Glicerinado | 6.44 |
| Galinha Pintadinha Extrato de Algodão e glicerina | 6.52 |
| Giovanna Baby Orange com Giby Care | 6.60 |
| Granado Glicerina | 6.98 |
| Huggies Turma da Mônica Cream Oil | 5.60 |
| Huggies Turma da Mônica Extra suave | 5.86 |
| Johnson's Hora de Brincar | 4.40 |
| Johnson's Baby recém-nascido | 5.86 |
| Muriel Baby Menina | 6.87 |
| Muriel Baby Menino | 7.20 |
| Natura Mamãe e Bebê Glicerina com óleo de passiflora | 7.83 |
| Panvel Baby Club | 6.64 |
| Patati Patata Extrato de Aloe Vera | 6.07 |
| Antibacterial bar soaps | |
| Dettol Cool | 11.26 |
| Dettol Cuidado Diário | 11.34 |
| Dettol Suave | 11.34 |
| Lifebuoy Aveia | 11.22 |
| Lifebuoy Care&Clinical 10 | 11.07 |
| Lifebuoy Cream | 11.10 |
| Lifebuoy Fresh | 11.25 |
| Lifebuoy Total | 11.24 |
| Protex Cream | 10.96 |
| Protex Erva doce | 11.05 |
| Protex Limpeza profunda | 10.28 |
| Protex Ômega 3 | 11.00 |
| Protex Própolis | 10.93 |
| Protex suave | 10.91 |
| Antibacterial liquid soaps | |
| Dettol original | 4.40 |
| Protex Cream | 5.90 |
| Lifebuoy | 9.50 |
| Syndet bars | |
| Eucerin Ph5 Syndet | 5.81 |
| La Roche Posay Lipikar Surgras | 10.35 |
| Liquid syndets | |
| Eucerin Pele Sensível pH5 Syndet | 5.30 |
| La Roche Posay Lipikar Surgras | 5.40 |
| Cetaphil Restoraderm | 5.93 |
| Fisiogel Sabonete Líquido Hidratante | 7.36 |
In the group of antibacterial soaps, 14 were bars and three were liquid soaps (Table 1). All bar soaps (100%) had pH>8.0; among the liquid soaps, 1 (33.3%) had pH<5.0; 1 (33.3%) had pH between 5.0 and 5.9 (33.3%), and 1 had pH>8.0. Only two antibacterial liquid soaps had the pH close to the physiological range.
In group of syndets, two were bar and four were liquid soaps (Table 1). Among the bar soaps, 1 (50%) had pH of 5.0–5.9, and 1 (50%) had pH>8.0; and among the three liquids soaps, 3 (75%) had pH between 5.0 and 5.9, and 1 (25%) had pH between 7.0 and 7.9.
When comparing the pH values between the liquid and bar soaps using Fisher's exact test, there was a statistically significant difference (p<0.0001), with the liquid soaps showing lower pH values (Fig. 1).
 variation according to the soap presentation n=90.")
When divided by soap category: children's soaps, antibacterial soaps, and syndets, different pH values were also found between them using the Kruskal–Wallis test (p=0.0017).
The multiple comparison test (Fisher's exact test) was used, which showed a statistically significant difference in pH (p=0.0032) between the children's soap and syndet groups, and between the antibacterial soap and syndet groups (p=0.0002). The syndets had significantly lower pH when compared to the others (p<0.05; Fig. 2). Only two of the assessed soaps had information on the label indicating the pH.
Discussion variation according to the group of soaps (children")
Skin pH alterations caused by the use of different types of soaps are well known.1,7,9,12,13 It is also known that skin pH is slightly acidic, and that highly-alkaline pH can damage the acid mantle that acts as an antibacterial barrier, as well as disrupt the lipid lamellae of the epidermis, resulting in skin dryness due to higher transepidermal water loss and allowing the entry of potential irritants and allergens.7,9,12,13 This occurs because the soap, in contact with water, undergoes a hydrolysis reaction, releasing the alkali contained in these products and increasing the skin pH to 10–11.12 Based on the results, it can be observed that the soaps in liquid form are the most appropriate for everyday use, especially in children and infants, whose skin is more delicate and sensitive.
As demonstrated in the present study, Volochtchuk et al.,12 in a study carried out at the same institution, have already shown significant differences in pH between liquid and bar soaps, but the study evaluated both adult and children's soaps. The bar soaps showed pH>6, with most between 9 and 10. As for the liquid soaps, most showed pH between 6 and 6.9.11
Liquid syndets have a pH closer to the physiological range (approximately 5), and are especially recommended to patients with diseases that alter the skin barrier (such as atopic dermatitis and ichthyosis) or children with sensitive skin. In these individuals, the use of soaps with high pH worsens xerosis and can generate solutions of continuity of the skin, which can be a gateway to pathogens. Syndet action occurs in two ways: first, by reducing the interaction between tensioactive agents and skin proteins and lipids; and second, by restoring lipids and moisturizing agents lost during the washing.19 Thus, the skin does not dry, remaining hydrated.
Antibacterial bar soaps showed the highest pH values of all assessed soaps. This demonstrates that these products can be aggressive to the child's skin and should not be routinely used, but only in specific situations and for short periods of time, and on restricted parts and not the entire body, preferably in liquid form.
It was verified that only two of the included soaps had any mention of pH levels on their package. The study by Tarun et al.22 mentioned that the labels of all assessed soaps, except for one, had no information related to the product pH. It was observed that even those products whose packaging contained phrases such as “neutral pH”, “balanced pH”, or “dermatologically tested” had pH above the expected range. Therefore, it was found that many of these products provide information that can confuse the consumer, since the fact that the skin is slightly acidic is not generally known by the public, as well as the importance of maintaining the skin's barrier function. Only one brand (Eucerin bar and liquid soap, Eucerin®, USA) displayed pH specification on the packaging, which makes it difficult to choose or recommend these products, by both the lay population and health professionals.
Most analyzed soaps are manufactured and sold in Brazil. Although some of them represent internationally-renowned brands, it cannot be verified that their chemical composition and hence their pH is the same worldwide. However, as this study selected product brands that are also available in other countries, in easily accessible and popular stores, and also because as many different brands as possible were acquired, it is believed that the results can be extrapolated to other cities in Brazil and other regions of the world, which should be supported by studies in these locations.
This study highlights the pH inadequacy of several children's products freely available in points of purchase. Pediatricians, parents, and caregivers should be aware of the characteristics of products used in pediatric patients, as some may even cause damage to the skin of children and infants.
Based on this fact, it is important that health surveillance institutions that regulate the selling of products for infant use establish stricter criteria for their commercialization, as well as for the information that should be included in their packaging, including the product pH.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Prof. Dr. Ana Lucia Tararthuch and Prof. Dr. Ricardo Perez for allowing the use of the facilities, machinery, and equipment of the Renal Physiology Laboratory of UFPR for measuring the pH of the products and UFPR statistician, Ricardo Petterle, for his contribution to the statistical analysis.
Please cite this article as: Mendes BR, Shimabukuro DM, Uber M, Abagge KT. Critical assessment of the pH of children's soap. J Pediatr (Rio J). 2016;92:290–5.




